

Latent TB Infection (LTBI) Testing in Vietnam
Vietnam: High-Burden Tuberculosis (TB) Country
Facts and Figures
high TB burden countries.
These 30 countries account for nearly 90% of world’s TB burden1
active TB cases2.
HIV & TB Co-infection
Leading cause of disease and death in the country despite enhanced provisioning of the antiretroviral therapy (ART) and isoniazid preventive therapy (IPT) that have helped to reduce the number of TB/HIV co-infected patients.3
causes of death worldwide4.
HIV associated deaths caused by MDR-TB in 2018 5.
People living with HIV more susceptible to active TB6.
Multi-drug Resistant TB (MDR-TB)
While Vietnam has made significant progress in reductions in TB incidence, prevalence, and mortality well before the Millennium Development Goal (MDG) 2015 target date, rising numbers of multidrug-resistant TB (MDR-TB) is still a major challenge.
highest MDR-TB burden countries.7
new cases annually1.
Latent TB Infection (LTBI) Testing
WHO has identified the need to detect, diagnose and treat latent TB infection (LTBI) as a key strategy to end TB. Testing is the first step to treat those who have LTBI to break the cycle of transmission and infection of TB.
But, when 25% of the world’s population have a prior infection of the Mycobacterium TB bacteria and remain asymptomatic8, and when 1 in 10 with LTBI progresses to active TB, ending TB needs to begin with an understanding of prioritising whom to screen.9
Who should get tested for LTBI?
Both the Tuberculin Skin Test (TST) and Interferon-gamma release assays (IGRA) tests, which include the T-SPOT .TB test are used to aid the detection of latent TB infection in Vietnam.
While the TST seems simple enough to perform and does not require phlebotomy, the clinical and operational limitations of the TST are well documented. Detection of LTBI using the TST is also a challenge to administer and interpret.
TST test and cross-reactivity with the BCG vaccine
In Vietnam, BCG is a vaccine used in the expanded immunization program to try and inoculate people against Tuberculosis. This means that almost all babies are vaccinated BCG. Not all vaccines work equally well, and the BCG has significant limitations in preventing the spread of TB.
TST uses mixture proteins, sometimes referred to as purified protein derivative (PPD), and these protein cross react with BCG and non-tuberculous Mycobacteria (NTM), leading to low specificity in patients with BCG vaccine. Low specificity means higher false positive results especially in children, which leads to overtreatment.10
Limitations with TST that are seen in BCG vaccinated populations absent when using IGRAs.
IGRAs are an in vitro diagnostic blood test, which detect interferon-gamma released by T cells after exposure to certain TB-specific antigens, as an indirect measure of adaptive cell immunity. The T-SPOT.TB test, which is a type of commercially-available IGRA test, uses TB-specific antigens ESAT-6 and CFP10. These antigens used are important because they are specific for MTB, and not present in the BCG vaccine or non-TB mycobacterium (NTM), limiting false reactions.
TB Guidelines: Vietnam
The Ministry of Health Vietnam, Decision 1313/QD-BYT: Guidelines for Detecting and Treating Latent TB, March 24, 2020¹¹.
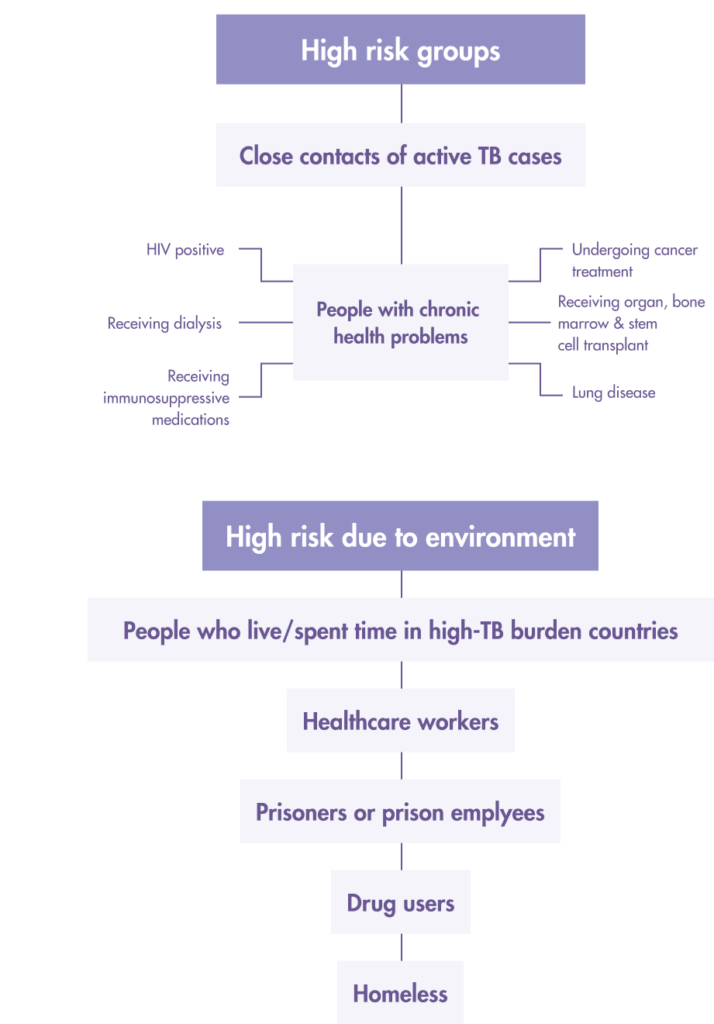
Prioritize Latent TB infection (LTBI) screening for “high risk” people from these two groups:
1. Close/Frequent contact with active TB patients
- Children < 5 years old have household contact with a TB patient Persons aged > 5 years and older who have household contact with a TB patients
- Healthcare workers in TB prevention units or at health facilities that may have TB patients
- Prison staff and prisoners
2. People with the following underlying health conditions
- People living with HIV (all ages)
- Pneumonia patient
- Diabetic patients
- Patients with renal impairment, hemodialysis
- Organ transplant and pre-organ transplant patients
- Patients on long-term immunosuppressive therapy (systemic disease eg: lupus, rheumatoid arthritis, psoriasis) and those treated with biologic drugs (anti-TNF)
LTBI screening and treatment based on these 2 factors:
1. A positive test Tuberculin/Mantoux Skin or The Interferon-Gamma Release Assay (IGRA) TB blood test.
- IGRA test for the detection of TB infection is based on the quantification of peripheral blood IFN-γ levels after activation by TB-specific antigens ESAT-6, CFP-10. There are two types of IGRA tests in use based on the following methods
- ELISPOT (enzyme-linked immunospot) e.g. T-SPOT.TB
- ELISA (enzyme-linked immune absorbent)
2. Exclusion of active TB by clinical examination that includes:
- Chest X-ray
- Sputum smear
- Abnormalities in Extrapulmonary organs suspected of TB
Begin LTBI treatment only when the above 2 factors are met to avoid incomplete treatment leading to multi-drug resistant TB (MDR-TB).
References
- WHO Global Tuberculosis Report, 2018. Available from: https://www.who.int/tb/publications/global_report/gtbr2018_main_text_28Feb2019.pdf?ua=1
- Press Release: The National Tuberculosis (TB) Program Partners with USAID to implement a new strategy to end TB in Vietnam.15 December, 2020. Available from: https://www.usaid.gov/vietnam/press-releases/dec-15-2020-national-tuberculosis-tb-program-partners-usaid-implement
- Q.M. Trinh, H.L. Nguyen, T.N. Do, V.N. Nguyen, B.H. Nguyen, T.V.A. Nguyen, V. Sintchenko, B.J. Marais (2016),Tuberculosis and HIV co-infection in Vietnam, International Journal of Infectious Diseases, Vol. 46, 56-60. Available from: https://www.sciencedirect.com/science/article/pii/S1201971216310086
- WHO Tuberculosis. Key Facts. 14 October 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis
- Lee, Joyce. “The Rise of Multidrug-Resistant Tuberculosis in HIV Patients”. Infectious Disease Advisor. (2021). Available from: https://www.infectiousdiseaseadvisor.com/home/topics/hiv-aids/multidrug-resistant-tb-is-serious-threat-especially-to-those-infected-with-hiv/
- Kwan CK, Ernst JD. HIV and tuberculosis: a deadly human syndemic. Clinical Microbiology Review. 2011 Apr;24(2):351-76. doi: 10.1128/CMR.00042-10. PMID: 21482729; PMCID: PMC3122491.
- World Health Organization. Global Tuberculosis Report, 2015. WHO; Geneva, Switzerland.
- Cohen A, Mathiasen VD, Schön T, Wejse C. The global prevalence of latent tuberculosis: a systematic review and meta-analysis. Eur Respir J. 2019 Sep 12;54(3):1900655. doi: 10.1183/13993003.00655-2019. PMID: 31221810.
- Centers for Disease Control and Prevention.Deciding when to treat latent TB Infection. Available from: https://www.cdc.gov/tb/topic/treatment/decideltbi.htm
- Spicer KB, Turner J, Wang SH, Koranyi K, Powell DA. Tuberculin skin testing and T-SPOT.TB in internationally adopted children. Pediatric Infectious Diseases J. 2015 Jun;34(6):599-603. doi: 10.1097/INF.0000000000000680. PMID: 25973937.
- Ministry of Health, Socialist Republic of Vietnam (24 March 2020). Issuance of Guidelines for Detecting and Treating Potential Tuberculosis (1313/QD-BYT). Available from: https://thuvienphapluat.vn/van-ban/The-thao-Y-te/Quyet-dinh-1313-QD-BYT-2020-Huong-dan-phat-hien-va-dieu-tri-lao-tiem-an-452472.asp
Latent TB infection (LTBI) detection:
Important to ending TB in Vietnam
In Vietnam, approximately 12,000 people die from TB every year, higher than the death toll from road accidents. Many patients die mainly because the disease is not discovered and treated in time. Preventative treatment that includes detecting and treating latent TB infection (LTBI) before the disease becomes active is instrumental in ending one of the key causes of death in the country.
Watch these videos to understand how T-SPOT.TB is critical to Vietnam’s End TB strategy.
Part 1: Priortise Latent TB Infection (LTBI) screening in Vietnam.
The latent TB infection (LTBI) population is large in high-TB incidence countries such as Vietnam. Find out from Dr Do Bang Tam, Hanoi Lung Hospital on how to prioritise LTBI screening as the first step to ending TB.
Part 2: Latent Tuberculosis Diagnostic Test and Treatment for Vietnam
According to Dr Do Bang Tam, Hanoi Lung Hospital, to break the chain of TB infection and transmission for BCG-vaccinated population such as Vietnam, using the right latent TB test is critical. Also, find out what the treatment plan is for those with latent TB infection (LTBI).
Part 3: What Does a Borderline T-SPOT.TB
Test Mean?
A borderline result is still a valid test result, but what does it mean? And why is there a need for a borderline test category? Dr Do Bang Tam, Hanoi Lung Hospital provides the technical details of the IGRA tests and why they should be used to aid the detection of TB amongst immunocompromised patients.
Why T-SPOT®.TB?
1 small tube. 1 million ways to find the truth¹
Developed by leading diagnostic company Oxford Immunotec, the T-SPOT.TB test is a single visit blood test for tuberculosis designed to reduce assay variability and maximize sensitivity, even in the immunocompromised.²
IGRA technology is based on the release of interferon-gamma secreted by individual effector T cells (both CD4+ and CD8+) after being stimulated by TB-specific antigens. The T-SPOT.TB test uses the enzyme-linked immunospot (ELISPOT) methodology to enumerate M. tuberculosis-sensitized T cells by capturing interferon-gamma in the vicinity of T cells from which it was secreted.
When your test looks for signs of TB infection using T cells, it matters how many T cells you include. The T-SPOT.TB test, unlike other tests, uses the same number each time. And it’s a big number: 250,000 cells per well, four wells per test¹. That’s a million witnesses to infection – and a moment of truth for TB.
How does the T-SPOT.TB test compare to other latent TB tests?
Learn more about the
T-SPOT.TB test
Learn More
The T-SPOT.TB test advantages

-
Accurate across patient populations1
- Immunosuppressed
- BCG vaccinated
-
Onl FDA-approved IGRA for children > 2 years2
-
Consistent results3
- Sensitivity: 98.8%
- Specificity: 99.1%
-
High test accuracy around result cut-off due to regulatory approved borderline zone – helping to prevent inappropriate therapy3, 4
Automation for the T-SPOT.TB test 3, 5
It is now possible to automate the T-SPOT.TB test using the CE-marked T-Cell Select™ reagent kit, giving more streamlined workflows, simplified sample logistics and freeing up technician’s time.
For everyone over the age of two
T-SPOT.TB: Only IGRA cleared by the US FDA for ages two and up1
When it comes to children, you know that not all diagnostic tests have the same accuracy in pediatric populations as they do in adults. Fortunately, the T-SPOT.TB test is reliable for not only the healthy children you test, but also for the children that have medical issues such as diabetes or are immunocompromised.

Contact Us
To find out more about T-SPOT.TB contact us:
Vietnam
Scitek Company
Hateco Building, Yen So,
Hoang Mai, Ha Noi
Vietnam
Email: sales@sciteck.vn
Phone: +84 901757600
Singapore
Oxford Immunotec Limited (Singapore Branch)
160 Robinson Road #23-03
SBF Center, Singapore 068914
Email: enquiry-RoA@oxfordimmunotec.com
Phone: +65 6246 6861
References
- Oxford Immunotec. T-SPOT.TB Package Insert PI-TB-IVD-UK-V3. Abingdon, UK. September 2020.
- Oxford Immunotec. T-SPOT.TB Package Insert TB-PI-US-0001 V9. Abingdon, UK. February 2021.
- Oxford Immunotec. T-SPOT.TB Package Insert PI-TB-IVD-UK-v3. Abingdon, UK. 2016.
- Oxford Immunotec. T-SPOT.TB Package Insert PI-TB-IVD-UK-v3. Abingdon, UK. 2016.Mazurek GH, Jereb J, Vernon A, LoBue P, Goldberg S, Castro K, IGRA Expert Committee, Centers for Disease Control and Prevention (CDC). Updated guidelines for using Interferon Gamma Release Assays to detect Mycobacterium tuberculosis infection – United States, 2010. MMWR Recomm Rep. 2010; 59(RR-5:1-25.
- Lewinsohn DM, Leonard MK, LoBue PA, et al. Official American ThoracicSociety/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. Clin Infect Dis. Published online December 8, 2016:ciw694. doi:10.1093/cid/ciw694
Việt Nam: Quốc gia có gánh nặng bệnh lao cao
Những con số và thực trạng
Nước có gánh nặng lao cao
Những quốc gia này chiếm khoảng gần 90% số ca Lao trên toàn thế giới1
Số ca nhiễm Lao hoạt động2
Đồng nhiễm Lao & HIV
Nguyên nhân chính gây ra các ca tử vong trong nước mặc dù việc tăng cường cung cấp điều trị ARV (ART) và điều trị dự phòng isoniazid (IPT) đã giúp giảm số ca đồng nhiễm Lao/HIV.³
Nguyên nhân tử vong trên toàn thế giới4
Số ca tử vong liên quan đến HIV
gây ra bởi Lao đa kháng (MDR-TB) trong năm 20185
Có khả năng
tiến triển thành lao hoạt động so với những người không nhiễm HIV6
Lao đa kháng (MDR-TB)
Mặc dù Việt Nam đã đạt được những bước tiến đáng kể trong việc giảm tỷ lệ mắc, tỷ lệ hiện mắc và tử vong do lao trước thời điểm hoàn thành Mục tiêu Phát triển Thiên niên kỷ (MDG) 2015, nhưng số lượng người mắc lao đa kháng (MDR-TB) ngày càng gia tăng vẫn là một thách thức lớn.
quốc gia có gánh nặng lao đa kháng cao nhất toàn cầu7
ca nhiễm mới hàng năm1
Xét nghiệm Lao tiềm ẩn (LTBI)
Tổ chức y tế thế giới (WHO) xác định việc nhận biết, chẩn đoán và điều trị lao tiềm ẩn là chiến lược quan trọng để chấm dứt bệnh lao. Xét nghiệm là bước đầu tiên để điều trị bệnh nhân lao tiềm ẩn nhằm phá vỡ chu trình lây truyền bệnh Lao.
Tuy nhiên, đến 25% dân số toàn cầu ở tình trạng nhiễm lao tiềm ẩn và hoàn toàn không có triệu chứng8, trong khi tỉ lệ diễn tiến thành lao hoạt động chỉ là 1 trên 10, mục tiêu kết thúc bệnh lao cần được bắt đầu với việc xác định rõ những nhóm bệnh nhân cần được ưu tiên sàng lọc lao tiềm ẩn.9
Những ai nên được sàng lọc lao tiềm ẩn?
Các phương pháp sàng lọc lao tiềm ẩn hiện có ở Việt Nam gồm xét nghiệm lao tố dưới da (TST) và xét nghiệm miễn dịch trung gian IGRA, trong đó có xét nghiệm T-SPOT.TB.
TST có ưu điểm là dễ thực hiện và không đòi hỏi phải lấy máu, tuy nhiên xét nghiệm này cũng có những hạn chế lâm sàng và thực hiện đã được ghi nhận rõ ràng. Việc sàng lọc lao tiềm ẩn bằng TST có những thách thức về quản lý và phiên giải kết quả.
Xét nghiệm TST có phản ứng chéo với vaccine BCG.
Ở Việt Nam, BCG được sử dụng trong Chương trình Tiêm chủng mở rộng, hầu hết trẻ em đều được chủng ngừa BCG. Không phải vaccine nào cũng có hiệu quả tốt, và BCG cũng có những hạn chế rõ ràng trong việc hạn chế sự lây lan của bệnh Lao.
TST sử dụng hỗn hợp protein tinh sạch từ môi trường nuôi cấy vi khuẩn Lao (PPD), những kháng nguyên này có phản ứng chéo với BCG và các vi khuẩn dòng Mycobacteria không gây lao khác (NTM), dẫn đến xét nghiệm này có độ đặc hiệu thấp ở nhóm có chủng ngừa BCG. Độ đặc hiệu thấp dẫn đến tỉ lệ dương tính giả cao, đặc biệt là ở trẻ em. Dương tính giả gây nên tình trạng điều trị không cần thiết, gây hại cho bệnh nhân, tốn kém10.
Những hạn chế này của xét nghiệm TST có thể được khắc phục khi sử dụng xét nghiệm IGRA.
IGRA là xét nghiệm máu In vitro (trong ống nghiệm), xác định lượng Interferron-gamma do tế bào T tiết ra sau khi được ủ với kháng nguyên đặc hiệu lao, là một dạng xét nghiệm đáp ứng miễn dịch trung gian. T-SPOT.TB là một trong những xét nghiệm IGRA tốt nhất, sử dụng các kháng nguyên ESAT-6 và CFP10, những kháng nguyên này đặc trưng cho vi khuẩn lao, đặc biệt là không có mặt trong thành phần vaccine BCG, vi khuẩn mycobacterium không lao (NTM), dẫn đến hạn chế những phản ứng dương tính giả.
Guidelines Lao tiềm ẩn của Việt Nam
Ngày 24/3/2020, Bộ Y tế đã ban hành Quyết định 1313/QĐ-BYT hướng dẫn phát hiện và điều trị lao tiềm ẩn.11
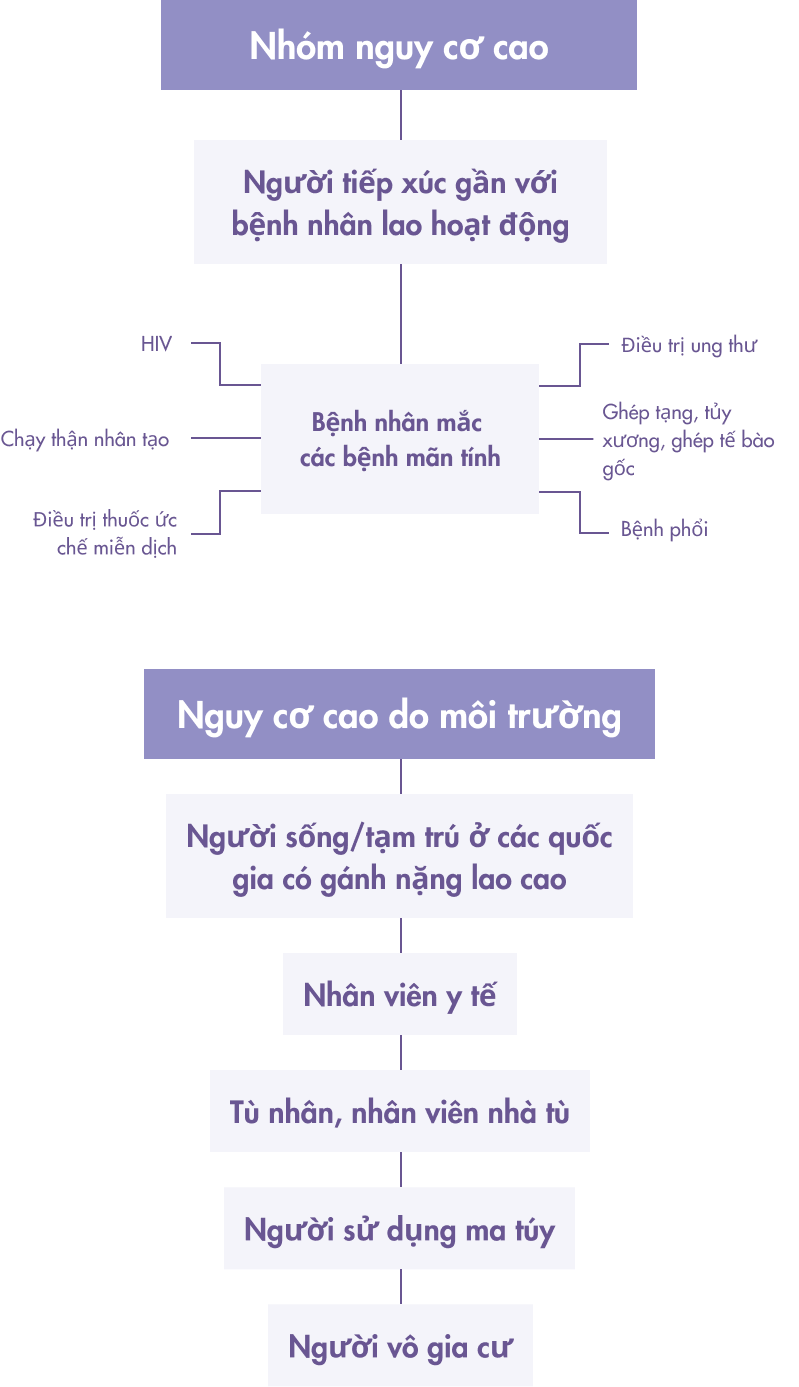
Ưu tiên sàng lọc Lao tiềm ẩn (LTBI) cho những người có “nguy cơ cao” gồm hai nhóm:
1. Nhóm tiếp xúc gần/thường xuyên với bệnh nhân Lao phổi:
- Trẻ em dưới 5 tuổi tiếp xúc hộ gia đình với bệnh nhân lao phổi
- Người từ 5 tuổi trở lên tiếp xúc hộ gia đình với bệnh nhân lao phổi
- Nhân viên y tế làm việc tại các đơn vị phòng chống lao cơ sở y tế có thể có bệnh nhân lao đến khám
- Tù nhân, quản giáo, nhân viên làm việc tại trại giam, trại giáo dưỡng
2. Nhóm người có các yếu tố làm tăng nguy cơ phát triển nhiễm lao thành bệnh lao:
- Người có HIV mọi lứa tuổi
- Bệnh nhân bụi phổi
- Bệnh nhân đái tháo đường
- Bệnh nhân suy thận, chạy thận nhân tạo
- Bệnh nhân cấy ghép tạng và người chuẩn bị cấy ghép tạng
- Bệnh nhân điều trị thuốc ức chế miễn dịch thường xuyên (bệnh tự miễn như lupus, viêm khớp dạng thấp, vẩy nến) và những bệnh nhân điều trị thuốc sinh học (anti-TNF)
Sàng lọc và điều trị lao tiềm ẩn dựa trên 2 yếu tố:
1. Xét nghiệm da Tuberculin/Mantoux hay xét nghiệm máu Interferon-Gamma Release Assay (IGRA) dương tính.
- Xét nghiệm IGRA phát hiện nhiễm Lao dựa trên sự định lượng IFN-y trong máu ngoại vi sau khi được kích hoạt bởi các kháng nguyên đặc hiệu của vi khuẩn Lao là ESAT-6, CFP-10. Có hai loại xét nghiệm IGRA được sử dụng dựa trên các phương pháp sau:
- ELISPOT ( enzyme liên kết điểm miễn dịch) VD: T-SPOT.TB
- ELISA ( enzyme liên kết miễn dịch hấp thụ)
2. Loại trừ lao hoạt động bằng khám lâm sàng, bao gồm:
- Chụp X quang phổi
- Nhuộm soi đờm
- Dấu hiệu bất thường ở cơ quang ngoài phổi nghi lao
Chỉ tiến hành điều trị lao tiềm ẩn khi thỏa mãn hai yếu tố trên để tránh việc điều trị không dứt điểm dẫn đến Lao kháng thuốc (MDR-TB).
References
- WHO Global Tuberculosis Report, 2018. Available from: https://www.who.int/tb/publications/global_report/gtbr2018_main_text_28Feb2019.pdf?ua=1
- Press Release: The National Tuberculosis (TB) Program Partners with USAID to implement a new strategy to end TB in Vietnam.15 December, 2020. Available from: https://www.usaid.gov/vietnam/press-releases/dec-15-2020-national-tuberculosis-tb-program-partners-usaid-implement
- Q.M. Trinh, H.L. Nguyen, T.N. Do, V.N. Nguyen, B.H. Nguyen, T.V.A. Nguyen, V. Sintchenko, B.J. Marais (2016),Tuberculosis and HIV co-infection in Vietnam, International Journal of Infectious Diseases, Vol. 46, 56-60. Available from: https://www.sciencedirect.com/science/article/pii/S1201971216310086
- WHO Tuberculosis. Key Facts. 14 October 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis
- Lee, Joyce. “The Rise of Multidrug-Resistant Tuberculosis in HIV Patients”. Infectious Disease Advisor. (2021). Available from: https://www.infectiousdiseaseadvisor.com/home/topics/hiv-aids/multidrug-resistant-tb-is-serious-threat-especially-to-those-infected-with-hiv/
- Kwan CK, Ernst JD. HIV and tuberculosis: a deadly human syndemic. Clinical Microbiology Review. 2011 Apr;24(2):351-76. doi: 10.1128/CMR.00042-10. PMID: 21482729; PMCID: PMC3122491.
- World Health Organization. Global Tuberculosis Report, 2015. WHO; Geneva, Switzerland.
- Cohen A, Mathiasen VD, Schön T, Wejse C. The global prevalence of latent tuberculosis: a systematic review and meta-analysis. Eur Respir J. 2019 Sep 12;54(3):1900655. doi: 10.1183/13993003.00655-2019. PMID: 31221810.
- Centers for Disease Control and Prevention.Deciding when to treat latent TB Infection. Available from: https://www.cdc.gov/tb/topic/treatment/decideltbi.htm
- Spicer KB, Turner J, Wang SH, Koranyi K, Powell DA. Tuberculin skin testing and T-SPOT.TB in internationally adopted children. Pediatric Infectious Diseases J. 2015 Jun;34(6):599-603. doi: 10.1097/INF.0000000000000680. PMID: 25973937.
- Ministry of Health, Socialist Republic of Vietnam (24 March 2020). Issuance of Guidelines for Detecting and Treating Potential Tuberculosis (1313/QD-BYT). Available from: https://thuvienphapluat.vn/van-ban/The-thao-Y-te/Quyet-dinh-1313-QD-BYT-2020-Huong-dan-phat-hien-va-dieu-tri-lao-tiem-an-452472.asp
Xét nghiệm lao tiềm ẩn (LTBI):
tầm quan trọng trong việc kết thúc bệnh Lao tại Việt Nam
Ở Việt Nam, có khoảng 12 000 người chết mỗi năm do bệnh lao, lớn hơn số người chết do tai nạn giao thông. Nhiều người chết vì không được phát hiện và điều trị sớm. Việc điều trị dự phòng bao gồm chẩn đoán và điều trị lao tiềm ẩn trước khi nó diễn tiến thành lao hoạt động là một biện pháp quan trọng để chấm dứt nguyên nhân gây tử vong ở nước ta.
Tham khảo video dưới đây về vai trò của xét nghiệm T-SPOT.TB trong Chiến lược Chấm dứt bệnh lao ở Việt Nam
Part 1: Ưu tiên sàng lọc lao tiềm ẩn (LTBI) ở Việt Nam.
Số người nhiễm lao tiềm ẩn là rất lớn ở những nước có gánh nặng lao cao như Việt Nam. Cùng bác sĩ Đỗ Băng Tâm, trưởng khoa Hóa Sinh Huyết học và Truyền máu Bệnh viện Phổi Hà Nội tìm hiểu tại sao ưu tiên sàng lọc lao tiềm ẩn lại là bước đầu tiên để kết thúc bệnh lao.
Part 2: Chẩn đoán và điều trị lao tiềm ẩn ở Việt Nam
Theo bác sĩ Đỗ Băng Tâm, để phá chu trình lây nhiễm ở quốc gia tiêm chủng BCG như Việt Nam, việc sử dụng đúng loại xét nghiệm sàng lọc lao tiềm ẩn là vấn đề cấp thiết. Đồng thời, hãy cùng tìm hiểu về liệu trình điều trị lao tiềm ẩn (LTBI).
Part 3: Kết quả “vùng xám” hay “chưa rõ ràng” của xét nghiệm T-SPOT.TB có ý nghĩa như thế nào?
Kết quả “chưa rõ ràng” vẫn là một kết quả hợp lệ, nhưng nó có ý nghĩa gì? Và tại sao cần có kết quả này trong bảng phiên giải kết quả T-SPOT.TB? Bác sĩ Đỗ Băng Tâm sẽ giải thích chi tiết hơn về mặt kỹ thuật của xét nghiệm IGRA và giải thích tại sao xét nghiệm này nên được sử dụng để chẩn đoán lao ở nhóm bệnh nhân suy giảm/ức chế miễn dịch.
TẠI SAO NÊN CHỌN XÉT NGHIỆM T-SPOT®.TB?
T-SPOT.TB: chỉ 1 ống nhỏ, 1 triệu cách để tìm chân lý¹
Được phát triển bởi công ty hàng đầu trong lĩnh vực xét nghiệm Oxford Immunotec, T-SPOT.TB là xét nghiệm sàng lọc lao chỉ cần một lần đến lấy máu, được thiết kế để giảm sai số đến mức thấp nhất và tối đa hóa độ nhạy, kể cả với nhóm bệnh nhân ức chế hay suy giảm miễn dịch²
Nguyên lý của xét nghiệm IGRA dựa trên sự giải phóng interferon-gamma được tiết ra bởi các tế bào T riêng lẻ (cả CD4 + và CD8 +) sau khi được kích thích bởi các kháng nguyên đặc hiệu của bệnh lao. Xét nghiệm T-SPOT.TB sử dụng phương pháp miễn dịch liên kết với enzym (ELISPOT) để đếm các tế bào T nhạy cảm với M. tuberculosis bằng cách bắt interferon-gamma trong vùng lân cận của các tế bào T mà nó được tiết ra.
Khi xét nghiệm của bạn tìm kiếm các dấu hiệu nhiễm lao bằng cách sử dụng tế bào T, điều quan trọng là bao gồm bao nhiêu tế bào T. Không giống như các xét nghiệm khác, T-SPOT.TB sử dụng một lượng tế bào được chuẩn hóa. Và đó là một con số lớn: 250.000 tế bào trên mỗi giếng, bốn giếng cho mỗi xét nghiệm1. Đó là một triệu nhân chứng cho nhiễm lao – và là một khoảnh khắc của sự thật đối với bệnh lao.
So sánh T-SPOT.TB với các xét nghiệm Lao tiềm ẩn khác?
Tìm hiểu thêm về xét nghiệm
T-SPOT.TB
TÌM HIỂU THÊM
Những ưu điểm của T-SPOT.TB
-
Độ chính xác cao hơn ở các nhóm bệnh nhân1
- Suy giảm miễn dịch
- Được tiêm vaccine BCG
-
Loại xét nghiệm IGRA duy nhất được FDA chấp thuận sử dụng cho trẻ > 2 tuổi2
- Thu lượng máu ít
- Không có phản ứng chéo với vacxin BCG
-
Kết quả nhất quán3
- Độ nhạy: 98.8%
- Độ đặc hiệu: 99.1%
-
Xét nghiệm có độ chính xác cao nhất quanh giá trị cut-off nhờ áp dụng cơ chế phiên giải kết quả “vùng xám” – giúp giảm thiểu việc điều trị do chẩn đoán sai 3,4
Khả năng thực hiện tự động hóa xét nghiệm T-SPOT.TB3,5
Hiện tại đã có thể thực hiện xét nghiệm T-SPOT.TB tự động hóa nhờ bộ kit T-Cell SelectTM. Cung cấp quy trình làm việc giản tiện hơn, đơn giản hóa việc vận chuyển mẫu và tiết kiệm thời gian thao tác
Xét nghiệm dành cho bệnh nhân từ 2 tuổi
T-SPOT.TB là xét nghiệm IGRA duy nhất được FDA phê chuẩn sử dụng cho trẻ từ 2 tuổi trở lên (các xét nghiệm IGRA thường từ 5 tuổi) 1
Khi thực hiện các xét nghiệm ở trẻ em, không phải xét nghiệm nào cũng có độ chính xác tương tự như ở người trưởng thành. May mắn là xét nghiệm T-SPOT.TB không chỉ có độ tin cậy cao ở những trẻ khỏe mạnh mà còn ở những trẻ có vấn đề về sức khỏe như trẻ mắc bệnh tiểu đường hay trẻ bị suy giảm/ức chế miễn dịch.
Liên hệ
To find out more about T-SPOT.TB contact us:
Vietnam
Tam Phat Pharma Export Import Trading Co. Ltd
Trung Lan Hamlet, Ba Diem Ward,
Hoc Mon District,
Ho Chi Minh City, Vietnam
Email: sonnv@tamphatco.com.vn
Phone: +84 901 757 600
Fax: +84 243 640 0631
Singapore
Oxford Immunotec Limited (Singapore Branch)
160 Robinson Road #23-03
SBF Center, Singapore 068914
Email: enquiry-RoA@oxfordimmunotec.com
Phone: +65 6246 6861
References
- Oxford Immunotec. T-SPOT.TB Package Insert PI-TB-IVD-UK-V3. Abingdon, UK. September 2020.
- Oxford Immunotec. T-SPOT.TB Package Insert TB-PI-US-0001 V9. Abingdon, UK. February 2021.
- Oxford Immunotec. T-SPOT.TB Package Insert PI-TB-IVD-UK-v3. Abingdon, UK. 2016.
- Oxford Immunotec. T-SPOT.TB Package Insert PI-TB-IVD-UK-v3. Abingdon, UK. 2016.Mazurek GH, Jereb J, Vernon A, LoBue P, Goldberg S, Castro K, IGRA Expert Committee, Centers for Disease Control and Prevention (CDC). Updated guidelines for using Interferon Gamma Release Assays to detect Mycobacterium tuberculosis infection – United States, 2010. MMWR Recomm Rep. 2010; 59(RR-5:1-25.
- Lewinsohn DM, Leonard MK, LoBue PA, et al. Official American ThoracicSociety/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. Clin Infect Dis. Published online December 8, 2016:ciw694. doi:10.1093/cid/ciw694