
Latent TB Infection (LTBI) Testing in Indonesia
Tuberculosis in Indonesia
Facts and Figures
Highest TB-burden country worldwide.1
Cause of death by a communicable, maternal, neonatal & nutritional disease.2
Highest cause of death in Indonesia aged 15 – 49 years.3
People died of TB in 2019.2
HIV & TB co-infection
People with active TB, co-infected with HIV in 2019.2
Increased HIV and TB co-infection from 2018 – 2019.2
Diabetes & TB co-infection
Leading cause of diabetes mellitus.4
People with diabetes by 2030.4
Diabetic TB patients shows drug resistance.4
Drug Resistant Tuberculosis (MDR-TB)
While Indonesia provides medication for all kinds of TB for free, many patients have cut short their treatments halfway due to drug resistance and recovery becomes more problematic5.
MDR-TB people in 2018.3
MDR-TB cases diagnosed in 2018.3
Diagnosed cases treated for MDR-TB.3
Latent TB Infection (LTBI) Testing
WHO has identified the need to detect, diagnose and treat latent TB infection (LTBI) as a key strategy to end TB. Testing is the first step to treat those who have LTBI to break the cycle of transmission and infection of TB.
But, when 25% of the world’s population have a prior infection of the Mycobacterium TB bacteria and remain asymptomatic6, and when 1 in 10 with LTBI progresses to active TB, ending TB needs to begin with an understanding of prioritising whom to screen7.
Who should get tested for LTBI?
Both the Tuberculin Skin Test (TST) and Interferon-gamma release assays (IGRA) tests, which include the T-SPOT®.TB test are used to aid the detection of latent TB infection in Indonesia.
While the TST seems simple enough to perform and does not require phlebotomy, the clinical and operational limitations of the TST are well documented. Detection of LTBI using the TST is also a challenge to administer and interpret.
TST test and cross-reactivity with the BCG vaccine
In Indonesia, BCG is a vaccine used in the expanded immunisation program to try and inoculate people against Tuberculosis. This means that almost all babies are vaccinated BCG. Not all vaccines work equally well, and the BCG has significant limitations in preventing the spread of TB.
TST uses mixture proteins, sometimes referred to as purified protein derivative (PPD), and these protein cross react with BCG and non-tuberculous Mycobacteria (NTM), leading to low specificity in patients with BCG vaccine. Low specificity means higher false positive results especially in children, which leads to overtreatment . TST uses mixture proteins, sometimes referred to as purified protein derivative (PPD), and these protein cross react with BCG and non-tuberculous Mycobacteria (NTM), leading to low specificity in patients with BCG vaccine. Low specificity means higher false positive results especially in children, which leads to overtreatment 8.
Limitations with TST that are seen in BCG vaccinated populations are absent when using IGRAs.
IGRAs are an in vitro diagnostic blood test, which detect interferon-gamma released by T cells after exposure to certain TB-specific antigens, as an indirect measure of adaptive cell immunity. The T-SPOT.TB test, which is a type of commercially-available IGRA test, uses TB-specific antigens ESAT-6 and CFP10. These antigens used are important because they are specific for MTB, and not present in the BCG vaccine or non-TB mycobacterium (NTM), limiting false reactions.
TB Guidelines: Indonesia
The Ministry of Health, Republic of Indonesia, Technical Instructions for Handling Latent Tuberculosis Infection, 2020.9
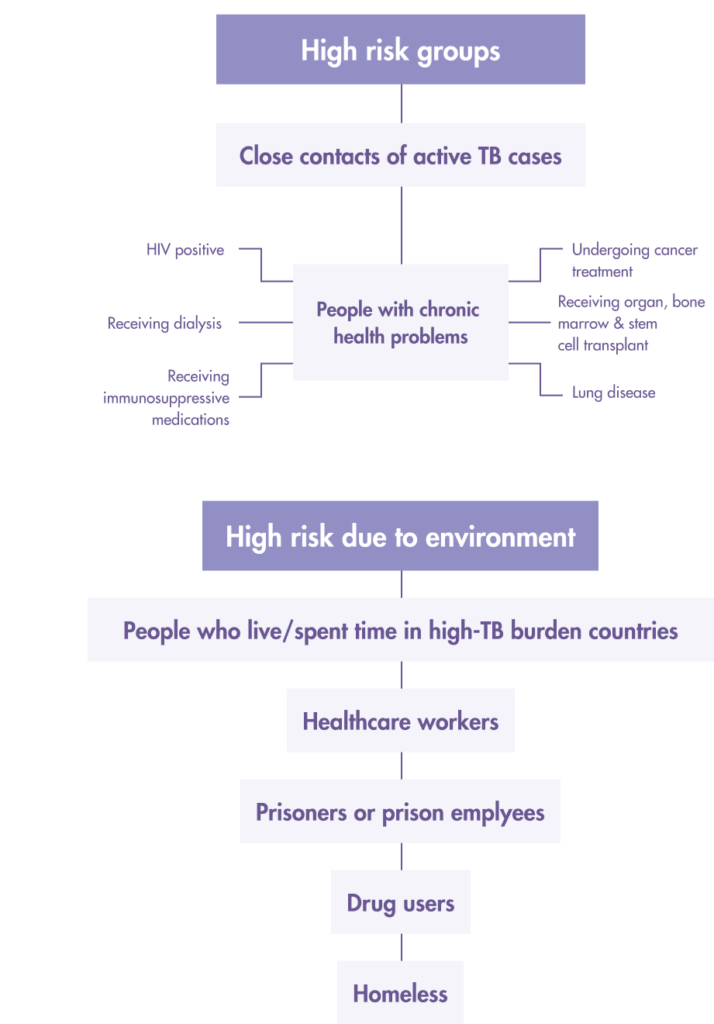
Prioritise latent TB infection (LTBI) screening for “high risk” people from these two groups:
1. People living with HIV/AIDS (ODHA)
2. Household contacts of those with confirmed pulmonary tuberculosis:
- Children < 5 years oldPneumonia patient
- Adolescents and adults > age 15 years
3. “At-risk” populations who are HIV-negative:
- Immunocompromised patients such as those undergoing the following treatment
- Cancer
- Dialysis
- Corticosteroids (long term)
- Patients who are preparing for organ transplants
- Healthcare workers
- Prison staff and prisoners
- Residents of boarding schools, military barracks
- Intravenous drug users
LTBI screening and treatment based on these 2 factors:
1. A positive test Tuberculin/Mantoux Skin or The Interferon-Gamma Release Assay (IGRA) TB blood test.
- IGRA test for the detection of TB infection is based on the quantification of peripheral blood IFN-γ levels after activation by TB-specific antigens ESAT-6, CFP-10. There are two types of IGRA tests in use based on the following methods:
- ELISPOT (enzyme-linked immunospot)e.g. T-SPOT.TB.
- ELISA (enzyme-linked immune absorbent).
2. Exclusion of active TB by clinical examination that includes:
- Chest X-ray
- Sputum smear
- Abnormalities in Extrapulmonary organs suspected of TB
Begin LTBI treatment only when the above 2 factors are met to avoid incomplete treatment leading to multi-drug resistant TB (MDR-TB).
References
- WHO: Global Tuberculosis Report 2020. 15 October 2020.
- StopTB Partnership & WHO. StopTB Partnership Dashboard: Tuberculosis Situation in 2019, Indonesia. Available from: http://www.stoptb.org/resources/cd/IDN_Dashboard.html
- USAID: Indonesia Tuberculosis Roadmap Overview, Fiscal Year 2021. Available from: https://www.usaid.gov/global-health/health-areas/tuberculosis/resources/news-and-updates/global-accelerator-end-tb/tb-roadmaps/indonesia
- Diabetes Mellitus Increases Risk of Multi-Drug Resistant Tuberculosis in Jakarta, Indonesia. I Fajarwati, D. Handayani, and E. Burhan C54. TUBERCULOSIS EPIDEMIOLOGY. May 1, 2019, A5153-A5153
- Cahya, Gemma. Indonesia struggles to tackle drug-resistant tuberculosis. The Jakarta Post. (July 21, 2019). Available from: https://www.thejakartapost.com/news/2019/07/21/indonesia-struggles-to-tackle-drug-resistant-tuberculosis.html
- Cohen A, Mathiasen VD, Schön T, Wejse C. The global prevalence of latent tuberculosis: a systematic review and meta-analysis. Eur Respir J. 2019 Sep 12;54(3):1900655. doi: 10.1183/13993003.00655-2019. PMID: 31221810.
- Centers for Disease Control and Prevention (2018). Deciding when to treat latent TB Infection. Available from: https://www.cdc.gov/tb/topic/treatment/decideltbi.htm
- Spicer KB, Turner J, Wang SH, Koranyi K, Powell DA. Tuberculin skin testing and T-SPOT.TB in internationally adopted children. Pediatric Infectious Diseases J. 2015 Jun;34(6):599-603. doi: 10.1097/INF.0000000000000680. PMID: 25973937.
- Kementerian Kesehatan Republik Indonesia. (2020) Petunjuk Teknis Penanganan Infeksi Laten Tuberculosis (ILTB). Available from: https://tbindonesia.or.id/wp-content/uploads/2021/01/Isi-Juknis-ILTB-FINAL-ok_published.pdf
Why T-SPOT®.TB?
1 small tube. 1 million ways to find the truth¹
Developed by leading diagnostic company Oxford Immunotec, the T-SPOT .TB test is a single visit blood test for tuberculosis designed to reduce assay variability and maximize sensitivity, even in the immunocompromised.²
IGRA technology is based on the release of interferon-gamma secreted by individual effector T cells (both CD4+ and CD8+) after being stimulated by TB-specific antigens. The T-SPOT.TB test uses the enzyme-linked immunospot (ELISPOT) methodology to enumerate M. tuberculosis-sensitized T cells by capturing interferon-gamma in the vicinity of T cells from which it was secreted.
When your test looks for signs of TB infection using T cells, it matters how many T cells you include. The T-SPOT.TB test, unlike other tests, uses the same number each time. And it’s a big number: 250,000 cells per well, four wells per test¹. That’s a million witnesses to infection – and a moment of truth for TB.
How does the T-SPOT.TB test compare to other latent TB tests?
Learn more about the T-SPOT.TB test
LEARN MOREThe T-SPOT.TB test advantages

-
Accurate across patient populations1
- Immunosuppressed
- BCG vaccinated
-
Onl FDA-approved IGRA for children > 2 years2
-
Consistent results3
- Sensitivity: 98.8%
- Specificity: 99.1%
-
High test accuracy around result cut-off due to regulatory approved borderline zone – helping to prevent inappropriate therapy3, 4
Automation for the T-SPOT.TB test 3, 5
It is now possible to automate the T-SPOT.TB test using the CE-marked T-Cell Select™ reagent kit, giving more streamlined workflows, simplified sample logistics and freeing up technician’s time.
For everyone over the age of two
T-SPOT.TB: Only IGRA cleared by the US FDA for ages two and up1
When it comes to children, you know that not all diagnostic tests have the same accuracy in pediatric populations as they do in adults. Fortunately, the T-SPOT.TB test is reliable for not only the healthy children you test, but also for the children that have medical issues such as diabetes or are immunocompromised.

Contact Us
To find out more about T-SPOT.TB contact us:
Indonesia
PT Oxford Imunotek Indonesia
Mixed Home Savoy B1 No. 36,
Jakarta Garden City, Cakung, Jakarta Timur
Email: info@oxford-indonesia.com
Phone: +62 8111712450
Singapore
Oxford Immunotec Limited (Singapore Branch)
160 Robinson Road #23-03
SBF Center, Singapore 068914
Email: enquiry-RoA@oxfordimmunotec.com
Phone: +65 6246 6861
References
- Oxford Immunotec. T-SPOT.TB Package Insert PI-TB-IVD-UK-V3. Abingdon, UK. September 2020.
- Oxford Immunotec. T-SPOT.TB Package Insert TB-PI-US-0001 V9. Abingdon, UK. February 2021.
- Oxford Immunotec. T-SPOT.TB Package Insert PI-TB-IVD-UK-v3. Abingdon, UK. 2016.
- Mazurek GH, Jereb J, Vernon A, LoBue P, Goldberg S, Castro K, IGRA Expert Committee, Centers for Disease Control and Prevention (CDC). Updated guidelines for using Interferon Gamma Release Assays to detect Mycobacterium tuberculosis infection – United States, 2010. MMWR Recomm Rep. 2010; 59(RR-5:1-25.
- Lewinsohn DM, Leonard MK, LoBue PA, et al. Official American ThoracicSociety/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. Clin Infect Dis. Published online December 8, 2016:ciw694. doi:10.1093/cid/ciw694
Gambaran: Tuberkulosis (TB) di Indonesia
Fakta dan Angka
Negara dengan beban TB tertinggi di dunia.1
Penyebab kematian penyakit menular, maternal, neonatal dan penyakit karena kekurangan gizi.2
Penyebab kematian tertinggi di Indonesia pada usia 15 – 49 tahun.3
Orang dengan TB aktif, koinfeksi HIV pada tahun 2019.2
Koinfeksi HIV & TB
Orang yang berkembang menjadi TB dan koinfeksi HIV pada tahun 2019.2
Peningkatan koinfeksi HIV dan TB dari 2018 – 2019.2
Diabetes dan koinfeksi TBC
Penyebab utama diabetes melitus.4
Orang dengan diabetes pada tahun 2030.4
Pasien TB diabetes menunjukkan resistensi obat.4
Tuberkulosis Resisten Obat (TB-MDR)
Sementara Indonesia menyediakan pengobatan untuk semua jenis TB secara gratis, banyak pasien yang mempersingkat pengobatan mereka di tengah jalan karena resistensi obat dan pemulihan menjadi lebih bermasalah5.
Penderita MDR-TB pada tahun 2018.3
Kasus MDR-TB yang terdiagnosis pada 2018. 3
Kasus terdiagnosis dan dirawat karena MDR-TB. 3
Pengujian Infeksi TB Laten (ILTB)
WHO telah mengidentifikasi kebutuhan untuk mendeteksi, mendiagnosis, dan mengobati infeksi Laten TB (ILTB) sebagai strategi utama untuk mengakhiri TB. Pengujian adalah langkah pertama untuk mengobati mereka yang memiliki ILTB untuk memutus siklus penularan dan infeksi TB.
Tetapi, ketika 25% dari populasi dunia memiliki infeksi bakteri Mycobacterium TB sebelumnya dan tetap asimtomatik6, dan ketika 1 dari 10 orang dengan ILTB berkembang menjadi TB aktif, mengeliminasi TB perlu dimulai dengan pemahaman tentang memprioritaskan siapa yang harus diskrining7.
Siapa yang harus dites untuk ILTB?
Tuberculin Skin Test (TST) dan Interferon-gamma release assays (IGRA), termasuk tes T-SPOT®.TB digunakan untuk membantu deteksi infeksi laten TB di Indonesia.
Sementara TST tampaknya cukup sederhana untuk dilakukan dan tidak memerlukan proses pengambilan darah, tetapi telah diketahui banyak keterbatasan klinis dan operasional TST. Deteksi ILTB menggunakan TST juga merupakan tantangan dalam pengelolaan dan interpretasi.
Tes TST dan reaktivitas silang dengan vaksin BCG
Di Indonesia, BCG adalah vaksin yang digunakan dalam program imunisasi yang diperluas untuk mencoba dan menginokulasi orang terhadap Tuberkulosis. Artinya hampir semua bayi divaksinasi BCG. Tidak semua vaksin bekerja dengan baik, dan BCG memiliki keterbatasan yang signifikan dalam mencegah penyebaran TB.
TST menggunakan protein campuran, kadang-kadang disebut sebagai turunan protein murni (PPD), dan protein ini bereaksi silang dengan BCG dan Mycobacteria (NTM) non-TB, yang menyebabkan spesifisitas rendah pada pasien dengan vaksin BCG. Spesifisitas rendah berarti hasil positif palsu akan lebih tinggi terutama pada anak-anak, yang mengarah pada pengobatan yang tidak diperlukan8.
Keterbatasan TST pada populasi yang divaksinasi BCG tidak terjadi pada saat menggunakan IGRA.
IGRA adalah tes darah diagnostik in vitro, yang mendeteksi interferon-gamma yang dilepaskan oleh sel T setelah terpapar antigen spesifik TB tertentu, sebagai pengukuran tidak langsung dari imunitas sel adaptif. Tes T-SPOT.TB, merupakan jenis tes IGRA yang tersedia secara komersial, menggunakan antigen spesifik TB ESAT-6 dan CFP10. Antigen yang digunakan ini penting dikarenakan spesifik untuk MTB, dan tidak ada dalam vaksin BCG atau mikobakterium non-TB (NTM), sehingga membatasi reaksi palsu.
Pedoman TB: Indonesia
Kementerian Kesehatan Republik Indonesia, Petunjuk Teknis Penanganan Infeksi Laten Tuberculosis (ILTB), 20209.
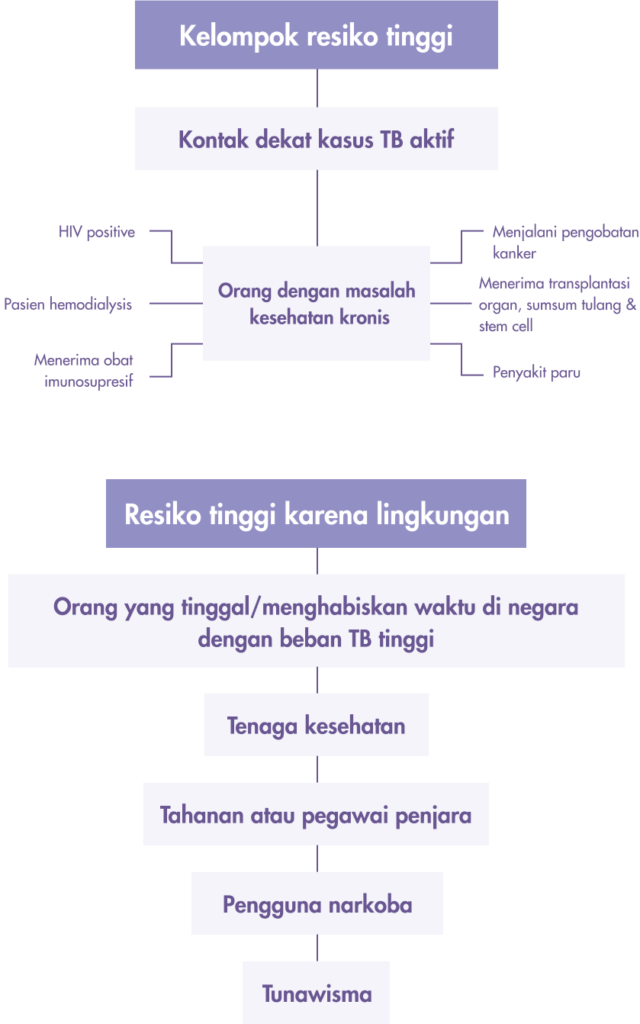
Berikut ini adalah kelompok risiko yang merupakan prioritas skrining infeksi TB Laten (LTBI) untuk orang “berisiko tinggi” adalah kelompok ini:
1. Orang dengan HIV/AIDS (ODHA)
2. Kontak serumah dengan pasien TBC paru yang terkonfirmasi bakteriologis
- Anak usia di bawah 5 tahun
- Remaja dan dewasa (usia di atas 15 tahun)
3. Kelompok risiko lainnya dengan hasil HIV negatif
- Pasien immunocompromised lainnya seperti:
- pasien yang menjalani pengobatan kanker
- pasien yang mendapatkan perawatan dialisis
- pasien yang mendapat kortikosteroid jangka panjang
- Pasien yang sedang menjalani persiapan transplantasi organ, dll).
- Petugas Kesehatan
- Petugas penjaga penjara dan tahanan
- Sekolah berasrama, barak militer
- Pengguna narkoba dengan jarum suntik
Skrining dan pengobatan ILTB berdasarkan 2 faktor ini:
1. Tes darah TB Tuberculin/Mantoux Skin positif atau The Interferon-Gamma Release Assay (IGRA).
- Tes IGRA untuk mendeteksi infeksi TB didasarkan pada kuantifikasi kadar IFN-γ darah tepi setelah aktivasi oleh antigen spesifik TB ESAT-6, CFP-10. Ada dua jenis tes IGRA yang digunakan berdasarkan metode berikut:
- ELISPOT (enzyme-linked immunospot) mis. T-SPOT.TB.
- ELISA (penyerap imun terkait enzim).
2. Pengecualian TB aktif dengan pemeriksaan klinis yang meliputi:
- Rontgen dada
- Apusan dahak
- Kelainan pada organ ekstra paru yang dicurigai TB
Mulailah pengobatan LTBI hanya jika 2 faktor di atas terpenuhi untuk menghindari pengobatan yang tidak lengkap yang mengarah ke TB yang resistan terhadap berbagai obat (MDR-TB).
References
- WHO: Global Tuberculosis Report 2020. 15 October 2020.
- StopTB Partnership & WHO. StopTB Partnership Dashboard: Tuberculosis Situation in 2019, Indonesia. Available from: http://www.stoptb.org/resources/cd/IDN_Dashboard.html
- USAID: Indonesia Tuberculosis Roadmap Overview, Fiscal Year 2021. Available from: https://www.usaid.gov/global-health/health-areas/tuberculosis/resources/news-and-updates/global-accelerator-end-tb/tb-roadmaps/indonesia
- Diabetes Mellitus Increases Risk of Multi-Drug Resistant Tuberculosis in Jakarta, Indonesia. I Fajarwati, D. Handayani, and E. Burhan C54. TUBERCULOSIS EPIDEMIOLOGY. May 1, 2019, A5153-A5153
- Cahya, Gemma. Indonesia struggles to tackle drug-resistant tuberculosis. The Jakarta Post. (July 21, 2019). Available from: https://www.thejakartapost.com/news/2019/07/21/indonesia-struggles-to-tackle-drug-resistant-tuberculosis.html
- Cohen A, Mathiasen VD, Schön T, Wejse C. The global prevalence of latent tuberculosis: a systematic review and meta-analysis. Eur Respir J. 2019 Sep 12;54(3):1900655. doi: 10.1183/13993003.00655-2019. PMID: 31221810.
- Centers for Disease Control and Prevention (2018). Deciding when to treat latent TB Infection. Available from: https://www.cdc.gov/tb/topic/treatment/decideltbi.htm
- Spicer KB, Turner J, Wang SH, Koranyi K, Powell DA. Tuberculin skin testing and T-SPOT.TB in internationally adopted children. Pediatric Infectious Diseases J. 2015 Jun;34(6):599-603. doi: 10.1097/INF.0000000000000680. PMID: 25973937.
- Kementerian Kesehatan Republik Indonesia. (2020) Petunjuk Teknis Penanganan Infeksi Laten Tuberculosis (ILTB). Available from: https://tbindonesia.or.id/wp-content/uploads/2021/01/Isi-Juknis-ILTB-FINAL-ok_published.pdf
Kenapa T-SPOT®.TB?
T-SPOT.TB: 1 tabung kecil. 1 juta cara untuk menemukan kebenaran.¹
Dikembangkan oleh perusahaan diagnostik terkemuka Oxford Immunotec, tes T-SPOT.TB adalah tes darah satu kali kunjungan untuk tuberkulosis yang dirancang untuk mengurangi variabilitas pengujian dan memaksimalkan sensitivitas, bahkan pada pasien dengan gangguan kekebalan.²
Teknologi IGRA didasarkan pada pelepasan interferon-gamma yang disekresikan oleh sel T efektor individu (baik CD4+ maupun CD8+) setelah dirangsang oleh antigen spesifik TB. Tes T-SPOT.TB menggunakan metodologi enzyme-linked immunospot (ELISPOT) untuk menghitung sel T tersensitisasi M. tuberculosis dengan menangkap interferon-gamma di sekitar sel T dari mana ia disekresikan.
Ketika tes Anda mencari tanda-tanda infeksi TB menggunakan sel T, penting berapa banyak sel T yang Anda sertakan. Tes T-SPOT.TB, tidak seperti tes lainnya, menggunakan nomor yang sama setiap kali. Dan itu jumlah yang besar: 250.000 sel per sumur, empat sumur per tes1. Itu adalah sejuta saksi infeksi – dan momen kebenaran untuk TB.
Bagaimana tes T-SPOT.TB dibandingkan dengan tes LTBI lainnya?
Pelajari lebih lanjut tentang tes T-SPOT.TB
KETAHUI LEBIH LANJUTKelebihan Tes T-SPOT.TB
-
Akurat di seluruh populasi pasien1
- Imunosupresi
- Vaksin BCG
-
Hanya IGRA yang disetujui FDA untuk anak-anak > 2 tahun2
-
Hasil yang konsisten3
- Sensitivitas: 98,8%
- Spesifisitas: 99,1%
-
Akurasi pengujian yang tinggi di sekitar hasil cut-off karena hasil borderline telah diakui – membantu mencegah terapi yang tidak tepat3, 4
Automation untuk the T-SPOT.TB test 3, 5
Sekarang pengujian T-SPOT.TB dapat diotomatisasi menggunakan kit reagen T-Cell Select™ bertanda CE, memberikan alur kerja yang lebih efisien, logistik sampel yang disederhanakan, dan meningkatkan efektifitas waktu tenaga analis.
Untuk semua orang yang berusia di atas dua tahun
T-SPOT.TB: Hanya IGRA yang disetujui oleh FDA AS untuk usia dua tahun ke atas1
Ketika menyangkut anak-anak, Anda tahu bahwa tidak semua tes diagnostik memiliki akurasi yang sama pada populasi anak-anak seperti pada orang dewasa. Untungnya, tes T-SPOT.TB dapat diandalkan tidak hanya untuk anak-anak sehat yang Anda tes, tetapi juga untuk anak-anak yang memiliki masalah medis seperti diabetes atau immunocompromised.
HUBUNGI KAMI
To find out more about T-SPOT.TB contact us:
Indonesia
PT Oxford Imunotek Indonesia
Mixed Home Savoy B1 No. 36,
Jakarta Garden City, Cakung, Jakarta Timur
info@oxford-indonesia.com
Email: info@oxford-indonesia.com
Phone: +62 8111712450
Singapore
Oxford Immunotec Limited (Singapore Branch)
160 Robinson Road #23-03
SBF Center, Singapore 068914
Email: enquiry-RoA@oxfordimmunotec.com
Phone: +65 6246 6861
References
- Oxford Immunotec. T-SPOT.TB Package Insert PI-TB-IVD-UK-V3. Abingdon, UK. September 2020.
- Oxford Immunotec. T-SPOT.TB Package Insert TB-PI-US-0001 V9. Abingdon, UK. February 2021.
- Oxford Immunotec. T-SPOT.TB Package Insert PI-TB-IVD-UK-v3. Abingdon, UK. 2016.
- Mazurek GH, Jereb J, Vernon A, LoBue P, Goldberg S, Castro K, IGRA Expert Committee, Centers for Disease Control and Prevention (CDC). Updated guidelines for using Interferon Gamma Release Assays to detect Mycobacterium tuberculosis infection – United States, 2010. MMWR Recomm Rep. 2010; 59(RR-5:1-25.
- Lewinsohn DM, Leonard MK, LoBue PA, et al. Official American ThoracicSociety/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. Clin Infect Dis. Published online December 8, 2016:ciw694. doi:10.1093/cid/ciw694