
Latent TB Infection (LTBI) Testing in Thailand
Tuberculosis in Thailand
Facts and Figures
Highest TB-burden country worldwide.1
Cause of death by a communicable, maternal, neonatal & nutritional disease.2
people died of TB in 2019.2
Decrease in TB deaths between 2018 – 2019.2
HIV & TB co-infection
Thailand’s 2017 – 2030 National AIDS Strategy outlines its plans to increase the integration of HIV health services with services for TB to close the co-infection gap3.
TB preventative therapy (TPT) works synergistically with, and independently of, antiretroviral therapy (ART) to reduce TB incidence amongst people living with HIV (PLHIV)4.
TB-HIV burden countries.5
New TB and HIV co-infection cases in 2019.2
TB and HIV co-infection cases in 2019.2
Drug Resistant Tuberculosis (DR-TB)
Thailand has transitioned out of WHO top 30 MDR-TB burden countries list in 20215.
New MDR-TB cases in 2019.2
Decrease MDR-TB cases between 2018 – 2019.2
Latent TB Infection (LTBI) Testing
WHO has identified the need to detect, diagnose and treat latent TB infection (LTBI) as a key strategy to end TB. Testing is the first step to treat those who have LTBI to break the cycle of transmission and infection of TB.
But, when 25% of the world’s population have a prior infection of the Mycobacterium TB bacteria and remain asymptomatic6, and when 1 in 10 with LTBI progresses to active TB, ending TB needs to begin with an understanding of prioritising whom to screen7.
Who should get tested for LTBI?
Both the Tuberculin Skin Test (TST) and Interferon-gamma release assays (IGRA) tests, which include the T-SPOT®.TB test are used to aid the detection of latent TB infection in Thailand.
While the TST seems simple enough to perform and does not require phlebotomy, the clinical and operational limitations of the TST are well documented. Detection of LTBI using the TST is also a challenge to administer and interpret.
TST test and cross-reactivity with the BCG vaccine
In Thailand, BCG is a vaccine used in the expanded immunization program to try and inoculate people against Tuberculosis. This means that almost all babies are vaccinated BCG. Not all vaccines work equally well, and the BCG has significant limitations in preventing the spread of TB.
TST uses mixture proteins, sometimes referred to as purified protein derivative (PPD), and these protein cross react with BCG and non-tuberculous Mycobacteria (NTM), leading to low specificity in patients with BCG vaccine. Low specificity means higher false positive results especially in children, which leads to overtreatment8.
Limitations with TST that are seen in BCG vaccinated populations are absent when using IGRAs.
IGRAs are an in vitro diagnostic blood test, which detect interferon-gamma released by T cells after exposure to certain TB-specific antigens, as an indirect measure of adaptive cell immunity. The T-SPOT.TB test, which is a type of commercially-available IGRA test, uses TB-specific antigens ESAT-6 and CFP10. These antigens used are important because they are specific for MTB, and not present in the BCG vaccine or non-TB mycobacterium (NTM), limiting false reactions.
TB Guidelines: Thailand
Division of Tuberculosis , The Ministry of Public Health Thailand: National Tuberculosis Control Programme Guideline, Thailand, 20189
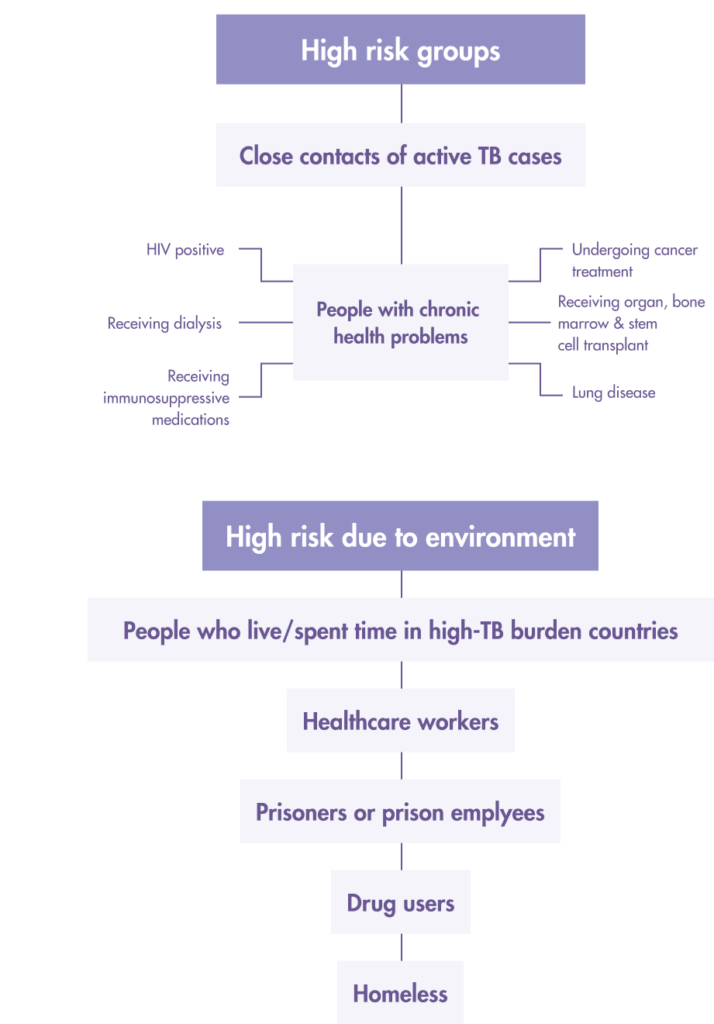
Prioritise Latent TB infection (LTBI) screening for “high risk” people from these two groups:
1. Close/Frequent contact with active TB patients
- Children < 5 years old have household contact with a TB patient.
- Persons aged > 5 years and older who have household contact with a TB patients.
- Healthcare workers in TB prevention units or at health facilities that may have TB patients.
- Prison staff and prisoners.
2. For latent TB infection (LTBI)
- People with the following underlying health conditions.
- People living with HIV (all ages).
- Pneumonia patient.
- Diabetic patients.
- Patients with renal impairment, hemodialysis.
- Organ transplant and pre-organ transplant patients.
- Patients on long-term immunosuppressive therapy (systemic disease eg: lupus, rheumatoid arthritis, psoriasis) and those treated with biologic drugs (anti-TNF).
LTBI screening and treatment based on these 2 factors:
1. A positive test Tuberculin/Mantoux Skin or The Interferon-Gamma Release Assay (IGRA) TB blood test.
- IGRA test for the detection of TB infection is based on the quantification of peripheral blood IFN-γ levels after activation by TB-specific antigens ESAT-6, CFP-10. There are two types of IGRA tests in use based on the following methods:
- ELISPOT (enzyme-linked immunospot)e.g. T-SPOT.TB.
- ELISA (enzyme-linked immune absorbent).
2. Exclusion of active TB by clinical examination that includes:
- Chest X-ray.
- Sputum smear.
- Abnormalities in Extrapulmonary organs suspected of TB.
Begin LTBI treatment only when the above 2 factors are met to avoid incomplete treatment leading to multi-drug resistant TB (MDR-TB).
References
- Tbthailand.org: Operational plan to end TB: 2017 – 2021.
- StopTB Partnership & WHO. StopTB Partnership Dashboard: Tuberculosis Situation in 2019, Thailand. Available from: http://www.stoptb.org/resources/cd/THA_Dashboard.html.
- UNAIDS (15 September 2017) Update: Thailand launches new national strategy to end the AIDS epidemic by 2030. Available on: https://www.unaids.org/en/resources/presscentre/featurestories/2017/september/20170915_Thailand_NSP.
- Akolo C, Adetifa I, Shepperd S, Volmink J. Treatment of latent tuberculosis infection in HIV infected persons. Cochrane Database Syst Rev. 2010;(1):Cd000171. Epub 2010/01/22. pmid:20091503.
- World Health Organization. WHO global lists of high burden countries for tuberculosis (TB), TB/HIV and multidrug/rifampicin-resistant TB (MDR/RR-TB), 2021–2025. Available from: https://www.who.int/news/item/17-06-2021-who-releases-new-global-lists-of-high-burden-countries-for-tb-hiv-associated-tb-and-drug-resistant-tb.
- Cohen A, Mathiasen VD, Schön T, Wejse C. The global prevalence of latent tuberculosis: a systematic review and meta-analysis. Eur Respir J. 2019 Sep 12;54(3):1900655. doi: 10.1183/13993003.00655-2019. PMID: 31221810.
- Centers for Disease Control and Prevention (2018). Deciding when to treat latent TB Infection. Available from: https://www.cdc.gov/tb/topic/treatment/decCenters for Disease Control and Prevention (2018). Deciding when to treat latent TB Infection. Available from: https://www.cdc.gov/tb/topic/treatment/decideltbi.htm.
- Spicer KB, Turner J, Wang SH, Koranyi K, Powell DA. Tuberculin skin testing and T-SPOT.TB in internationally adopted children. Pediatric Infectious Diseases J. 2015 Jun;34(6):599-603. doi: 10.1097/INF.0000000000000680. PMID: 25973937.
- Thailand, Ministry of Health, 2018. National Tuberculosis Control Program Guideline, Thailand 2018. Department of Disease Control, Tuberculosis Bureau. 614.542. ISBN 978-616-11-3670-3.
Why T-SPOT®.TB?
1 small tube. 1 million ways to find the truth¹
Developed by leading diagnostic company Oxford Immunotec, the T-SPOT.TB test is a single visit blood test for tuberculosis designed to reduce assay variability and maximize sensitivity, even in the immunocompromised.²
IGRA technology is based on the release of interferon-gamma secreted by individual effector T cells (both CD4+ and CD8+) after being stimulated by TB-specific antigens. The T-SPOT.TB test uses the enzyme-linked immunospot (ELISPOT) methodology to enumerate M. tuberculosis-sensitized T cells by capturing interferon-gamma in the vicinity of T cells from which it was secreted.
When your test looks for signs of TB infection using T cells, it matters how many T cells you include. The T-SPOT.TB test, unlike other tests, uses the same number each time. And it’s a big number: 250,000 cells per well, four wells per test¹. That’s a million witnesses to infection – and a moment of truth for TB.
How does the T-SPOT.TB test compare to other latent TB tests?
Learn more about the T-SPOT.TB test
LEARN MOREThe T-SPOT.TB test advantages

-
Accurate across patient populations1
- Immunosuppressed
- BCG vaccinated
-
Onl FDA-approved IGRA for children > 2 years2
-
Consistent results3
- Sensitivity: 98.8%
- Specificity: 99.1%
-
High test accuracy around result cut-off due to regulatory approved borderline zone – helping to prevent inappropriate therapy3, 4
Automation for the T-SPOT.TB test 3, 5
It is now possible to automate the T-SPOT.TB test using the CE-marked T-Cell Select™ reagent kit, giving more streamlined workflows, simplified sample logistics and freeing up technician’s time.
For everyone over the age of two
T-SPOT.TB: Only IGRA cleared by the US FDA for ages two and up1
When it comes to children, you know that not all diagnostic tests have the same accuracy in pediatric populations as they do in adults. Fortunately, the T-SPOT.TB test is reliable for not only the healthy children you test, but also for the children that have medical issues such as diabetes or are immunocompromised.

Contact Us
To find out more about T-SPOT.TB contact us
Thailand
Biomed Diagnostics (Thailand) Co., Ltd.
1518/4 Kengrungruengchai Bldg.,
7th Fl., Pracharaj Sai 1 Rd.,
Wongsawang, Bangsue, Bangkok 10800
Email: sales-diag@biomedthai.com
Phone: +66 02 5870256 58
Singapore
Oxford Immunotec Limited (Singapore Branch)
160 Robinson Road #23-03
SBF Center, Singapore 068914
Email: enquiry-RoA@oxfordimmunotec.com
Phone: +65 6246 6861
References
- Oxford Immunotec. T-SPOT.TB Package Insert PI-TB-IVD-UK-V3. Abingdon, UK. September 2020.
- Oxford Immunotec. T-SPOT.TB Package Insert TB-PI-US-0001 V9. Abingdon, UK. February 2021.
- Oxford Immunotec. T-SPOT.TB Package Insert PI-TB-IVD-UK-v3. Abingdon, UK. 2016.
- Mazurek GH, Jereb J, Vernon A, LoBue P, Goldberg S, Castro K, IGRA Expert Committee, Centers for Disease Control and Prevention (CDC). Updated guidelines for using Interferon Gamma Release Assays to detect Mycobacterium tuberculosis infection – United States, 2010. MMWR Recomm Rep. 2010; 59(RR-5:1-25.
- Lewinsohn DM, Leonard MK, LoBue PA, et al. Official American ThoracicSociety/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. Clin Infect Dis. Published online December 8, 2016:ciw694. doi:10.1093/cid/ciw694
วัณโรคในประเทศไทย
ภาพรวมและสถิติ
ประเทศที่มีภาระด้านวัณโรคเป็นอันดับสูงสุดของโลก1
สาเหตุการตาย ในกลุ่มโรคติดต่อ โรคที่ได้รับการถ่ายทอดจากแม่สู่ลูก โรคที่เป็นแต่กำเนิด และโรคที่เกิดจากภาวะโภชนาการ2
จำนวนผู้เสียชีวิตจากวัณโรคในปี 20192
อัตราการตายจากวัณโรคลดลง ในระหว่างปี 2018-20192
การติดเชื้อร่วมกันของผู้ป่วยโรคเอดส์และวัณโรค
ประเทศไทยได้จัดทำแผนปฏิบัติการระดับชาติด้านการต่อต้านวัณโรค 2017 – 2030 เพื่อให้สอดคล้องกับยุทธศาสตร์ยุติวัณโรคของสหประชาชาติ3
หนึ่งในยุทธศาสตร์นั้นได้กำหนดให้เร่งรัดการดำเนินงานผสมผสานวัณโรคและโรคเอดส์ ทั้งด้านการวางแผนงานร่วมกัน การเร่งค้นหา การให้ยาป้องกันวัณโรค การให้ยาป้องกันโรคติดเชื้อฉวยโอกาส และการให้ยาต้านไวรัสในผู้ป่วยวัณโรคทุกรายที่ติดเชื้อเอชไอวีร่วมด้วย4
ประเทศที่มีภาระผสมผสานด้านโรคเอดส์และวัณโรคมากที่สุด5
จำนวนผู้ป่วยวัณโรคร่วมกับการติดเชื้อเอชไอวีในปี 20192
ในกลุ่มผู้ที่เป็นวัณโรคร่วมกับการติดเชื้อเอชไอวี2
วัณโรคดื้อยา
ในปี 2021 ประเทศไทยมีภาระด้านวัณโรคดื้อยาอยู่ใน 30 อันดับสูงสุดของ WHO5
จำนวนผู้ป่วยวัณโรคดื้อยาเพิ่มในปี 20192
อัตราการเป็นวัณโรคดื้อยาลดลง ในระหว่างปี 2018 – 20192
การตรวจหาวัณโรคระยะแฝง
องค์การอนามัยโลกได้กำหนดยุทธศาสตร์ยุติวัณโรค โดยมุ่งเน้นในการตรวจหาและรักษาวัณโรคระยะแฝง การตรวจหาวัณโรคระยะแฝงให้พบจึงถือเป็นด่านแรกที่จะนำไปสู่การรักษา เพื่อยุติวงจรการถ่ายทอดและการติดเชื้อวัณโรค
แต่เมื่อ 25% ของประชากรโลกยังถูกคาดว่ามีการติดเชื้อ Mycobacterium หรือ TB โดยที่ยังไม่แสดงอาการ6 และ 1 ใน 10 ของคนที่มีวัณโรคระยะแฝงเหล่านี้จะพัฒนาไปเป็นวัณโรค การยุติวัณโรคจึงจำเป็นจะต้องเริ่มจากความเข้าใจว่าใครบ้างจำเป็นที่จะต้องตรวจและจำเป็นมากน้อยเพียงใด7
ใครบ้างที่ควรจะตรวจหาวัณโรคระยะแฝง
การทดสอบวัณโรคระยะแฝงในประเทศไทยมีทั้งการทดสอบทางผิวหนัง Tuberculin skin test (TST) และการทดสอบ Interferon-gamma release assays (IGRA) ซึ่งรวมถึง T-SPOT®.TB
ในขณะที่ TST เป็นการทดสอบที่สามารถทำได้ง่าย และไม่จำเป็นต้องเจาะเลือด แต่เป็นที่ทราบกันดีว่าข้อจำกัดของ TST อาจทำให้เกิดคำถามในการบันทึกและแปลผล
การทดสอบด้วย TST และการเกิด cross-reactivity จากวัคซีน BCG
ถึงแม้ว่า BCG จัดเป็นวัคซีนพื้นฐานที่ต้องฉีดให้เด็กไทยแรกเกิดทุกคน แต่ไม่แน่ว่าวัคซีนทุกชนิดใช่จะทำงานได้ดีเสมอไป รวมทั้งที่ผ่านมา BCG ก็มีข้อจำกัดอย่างมีนัยสำคัญในการป้องกันการแพร่ระบาดของวัณโรค
การทดสอบด้วย TST มักใช้โปรตีน purified protein derivative (PPD) เป็นตัวกระตุ้น ซึ่ง PPD มีปฏิกิริยา cross reaction ทั้งกับวัคซีน BCG และ non-tuberculous Mycobacteria (NTM) ทำให้การทดสอบด้วย TST มีความจำเพาะต่ำในผู้ที่เคยได้รับวัคซีน BCG มาก่อน ซึ่งหมายความว่า TST จะให้ผลบวกลวงได้มากกว่าปกติโดยเฉพาะในเด็ก ซึ่งจะนำไปสู่การรักษาที่มากเกินจำเป็น8
ข้อจำกัดเหล่านี้จากการตรวจหาวัณโรคระยะแฝงด้วย TST ในผู้ที่เคยได้รับวัคซีน BCG จะไม่เป็นข้อจำกัดอีกต่อไปเมื่อใช้การทดสอบด้วยวิธี IGRA
IGRA เป็นการตรวจเลือดโดยตรวจหา interferon-gamma ที่ถูกหลั่งออกมาจาก T-cells เมื่อถูกกระตุ้นด้วยแอนติเจนที่จำเพาะต่อเชื้อ TB ซึ่งเป็นการตรวจปฏิกิริยาที่เกิดจาก adaptive cell immunity
T-SPOT®.TB เป็นชุดตรวจ IGRA ที่ใช้ แอนติเจนที่จำเพาะต่อเชื้อ TB 2 ชนิด คือ ESAT-6 และ CFP-10 ซึ่งทั้ง 2 ชนิดมีความจำเพาะต่อเชื้อ TB อย่างมากและไม่มีอยู่ในวัคซีน BCG หรือเชื้อ NTM ดังนั้น จึงช่วยลดผลการทดสอบที่เป็นผลบวกลวง (false positive) จากวัคซีน BCG หรือการติดเชื้อ NTM
TB Guidelines: Thailand
แนวทางการควบคุมวัณโรคประเทศไทย พ.ศ. 2561 = National Tuberculosis Control Programme Guideline, Thailand 2018.– กรุงเทพฯ : สำนักวัณโรค กรมควบคุมโรค, 25619
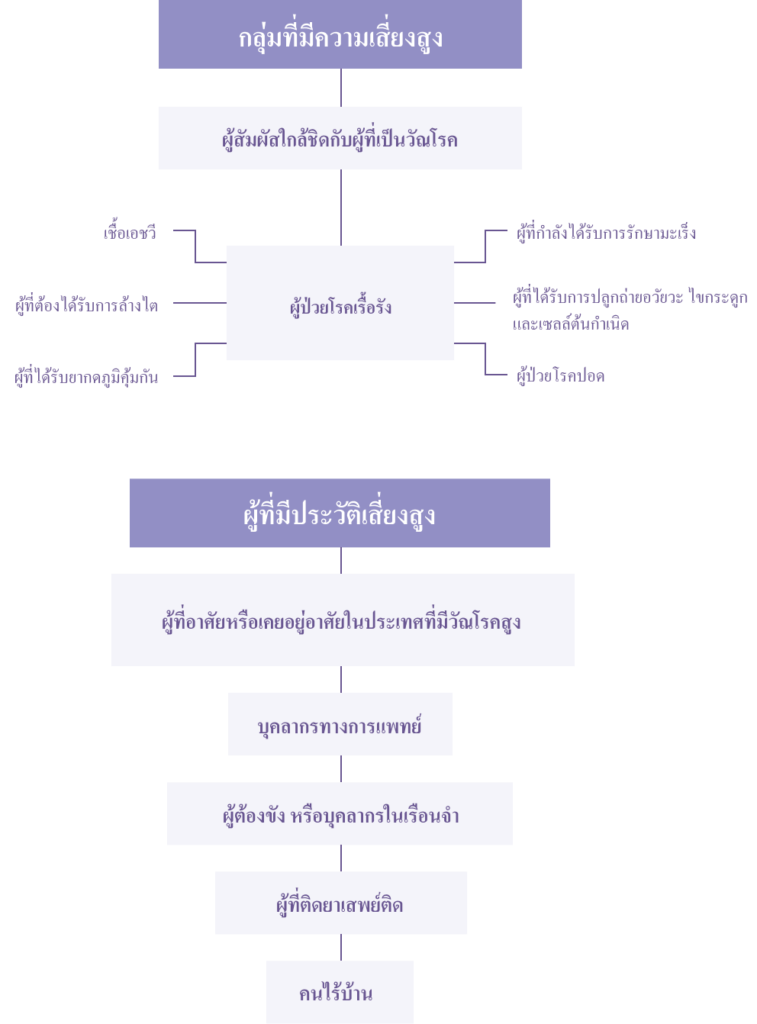
ให้ความสำคัญกับการคัดกรองวัณโรคระยะแฝง ในกลุ่มที่มีความเสี่ยงสูงสองกลุ่มนี้:
1. สัมผัสหรือใกล้ชิดกับผู้ป่วยวัณโรค
- เด็กอายุน้อยกว่า 5 ปี ในบ้านที่มีผู้ป่วยวัณโรค
- คนอายุมากกว่า 5 ปี ในบ้านที่มีผู้ป่วยวัณโรค
- บุคลากรทางการแพทย์ในหน่วยป้องกันวัณโรคที่มีผู้ป่วยวัณโรค
- เจ้าหน้าที่เรือนจำและผู้ต้องขัง
2. ผู้ที่มีภาวะร่างกายดังนี้
- คนมีเชื้อเอชไอวี
- ผู้ป่วยโรคปอดบวม
- ผู้ป่วยโรคเบาหวาน
- ผู้ป่วยโรคไตวาย ต้องฟอกไต
- ผู้ป่วยปลูกถ่ายอวัยวะและก่อนปลูกถ่ายอวัยวะ
- ผู้ป่วยที่ได้รับยากดภูมิคุ้มกันเป็นเวลานาน
การคัดกรองวัณโรคระยะแฝงและการรักษาขึ้นอยู่กับ 2 ปัจจัยนี้:
1. การตรวจ Tuberculin/Mantoux Skin หรือ Interferon-Gamma Release Assay (IGRA) ที่ผลเป็นบวก
- การตรวจ IGRA เพื่อตรวจหาเชื้อวัณโรคขึ้นอยู่กับปริมาณของระดับ IFN-γในเลือดหลังจากการกระตุ้นด้วยแอนติเจนจำเพาะ ESAT-6, CFP-10 มีตรวจ IGRA อยู่ 2 ประเภท:
- ELISPOT (enzyme-linked immunospot) เช่น T-SPOT.TB
- ELISA (enzyme-linked immune absorbent)
2. การคัดกรองออกของโรควัณโรค โดยการตรวจร่างกายดังนี้:
- เอกซ์เรย์ทรวงอก
- ตรวจเสมหะ
- ดูความผิดปกติในอวัยวะนอกจากปอดที่สงสัยว่าเป็นวัณโรค
เริ่มการรักษาวัณโรคระยะแฝง(LTBI )เมื่อมีปัจจัยทั่ง 2 ข้อ เพื่อหลีกเหลี้ยงการรักษาที่ไม่สมบูรณ์ซึ่งนำไปสู่วัณโรคดื้อยา (MDR-TB)
References
- Tbthailand.org: Operational plan to end TB: 2017 – 2021.
- StopTB Partnership & WHO. StopTB Partnership Dashboard: Tuberculosis Situation in 2019, Thailand. Available from: http://www.stoptb.org/resources/cd/THA_Dashboard.html.
- UNAIDS (15 September 2017) Update: Thailand launches new national strategy to end the AIDS epidemic by 2030. Available on: https://www.unaids.org/en/resources/presscentre/featurestories/2017/september/20170915_Thailand_NSP.
- Akolo C, Adetifa I, Shepperd S, Volmink J. Treatment of latent tuberculosis infection in HIV infected persons. Cochrane Database Syst Rev. 2010;(1):Cd000171. Epub 2010/01/22. pmid:20091503.
- World Health Organization. WHO global lists of high burden countries for tuberculosis (TB), TB/HIV and multidrug/rifampicin-resistant TB (MDR/RR-TB), 2021–2025. Available from: https://www.who.int/news/item/17-06-2021-who-releases-new-global-lists-of-high-burden-countries-for-tb-hiv-associated-tb-and-drug-resistant-tb.
- Cohen A, Mathiasen VD, Schön T, Wejse C. The global prevalence of latent tuberculosis: a systematic review and meta-analysis. Eur Respir J. 2019 Sep 12;54(3):1900655. doi: 10.1183/13993003.00655-2019. PMID: 31221810.
- Centers for Disease Control and Prevention (2018). Deciding when to treat latent TB Infection. Available from: https://www.cdc.gov/tb/topic/treatment/decCenters for Disease Control and Prevention (2018). Deciding when to treat latent TB Infection. Available from: https://www.cdc.gov/tb/topic/treatment/decideltbi.htm.
- Spicer KB, Turner J, Wang SH, Koranyi K, Powell DA. Tuberculin skin testing and T-SPOT.TB in internationally adopted children. Pediatric Infectious Diseases J. 2015 Jun;34(6):599-603. doi: 10.1097/INF.0000000000000680. PMID: 25973937.
- Thailand, Ministry of Health, 2018. National Tuberculosis Control Program Guideline, Thailand 2018. Department of Disease Control, Tuberculosis Bureau. 614.542. ISBN 978-616-11-3670-3.
ทำไมถึงต้องเป็น T-SPOT®.TB
T-SPOT®.TB: 1 หลอดเล็ก 1 ล้านหนทางค้นหา1
บริษัท Oxford Immunotec ผู้นำในด้านการตรวจวินิจฉัย ได้พัฒนาชุดตรวจ T-SPOT®.TB ซึ่งเป็นชุดตรวจเลือดเพื่อวินิจฉัยการติดเชื้อวัณโรคใน 1 visit โดยออกแบบขึ้นมาเพื่อลดความแปรผันในการทดสอบ และเพื่อเพิ่มความไวของการทดสอบให้มากที่สุด แม้ในผู้ที่มีภาวะภูมิคุ้มกันไม่ปกติ2
การตรวจ IGRA อาศัยหลักการปล่อย interferon-gamma ที่ถูกหลั่งออกมาโดยเซลล์ T cell effector ในแต่ละเซลล์ (ทั้ง CD4+ และ CD8+) ภายหลังจากที่ถูกกระตุ้นด้วยแอนติเจนที่จำเพาะต่อเชื้อ TB ชุดตรวจ T-SPOT®.TB ใช้เทคนิค enzyme-linked immunospot (ELISPOT) ในการนับ T cell ที่ไวต่อเชื้อ TB โดยจะทำการจับ interferon-gamma ที่ถูกหลั่งออกมาอยู่โดยรอบ T cell นั้นไว้
ในเมื่อเราตรวจหาสัญญาณการติดเชื้อวัณโรคด้วย T cell จำนวนของ T cell ที่ถูกนำมาใช้ในการทดสอบย่อมมีผลต่อการทดสอบไม่มากก็น้อย สิ่งที่ทำให้ชุดตรวจ T-SPOT®.TB ไม่เหมือนกับชุดทดสอบอื่นๆ คือ T-SPOT®.TB จะใช้จำนวน T cell เท่ากันทุกครั้ง โดยใช้เซลล์จำนวน 250,000 เซลล์ต่อหลุมทดสอบ โดยจะทดสอบทั้งหมด 4 หลุมสำหรับตัวอย่าง 1 ตัวอย่าง จึงเท่ากับมีเซลล์หนึ่งล้านเซลล์ร่วมเป็นพยานในการตรวจหาวัณโรคในทุกๆครั้ง
ชุดตรวจ T-SPOT.TB แตกต่างจากการทดสอบวัณโรคระยะแฝงด้วยวิธีอื่นๆ อย่างไร
อ่านเพิ่มเติมเรื่อง T-SPOT.TB
เรียนรู้เพิ่มเติมข้อดีของชุดตรวจ T-SPOT®.TB
-
มีความแม่นยำแม้ในกลุ่มผู้ป่วย1
- ผู้ที่ทานยากดภูมิ
- ผู้ที่เคยได้รับวัคซีน BCG
-
เป็น IGRA เพียงยี่ห้อเดียวที่ได้รับการยอมรับจาก US FDA ว่าสามารถใช้ในเด็กที่อายุมากกว่า 2 ปีได้ 2
-
ผลการทดสอบที่เหนือกว่า3
- ความไวในการทดสอบ 98.8%
- ความจำเพาะต่อเชื้อ 99.1%
-
ความแม่นยำสูง เนื่องจากมี borderline zone ที่ได้รับการยอมรับว่า สามารถช่วยป้องกันการรักษาที่ไม่เหมาะสมในคนไข้ได้3, 4。
ระบบอัตโนมัติสำหรับชุดตรวจ T-SPOT®.TB3, 5
ปัจจุบัน T-SPOT.TB สามารถใช้งานกับเครื่องอัตโนมัติได้ โดยใช้ร่วมกับน้ำยา T-Cell Select™ ซึ่งได้รับเครื่องหมาย CE เพื่อเพิ่มขีดความสามารถในการทดสอบตัวอย่างจำนวนมาก ช่วยยืดเวลาส่งตัวอย่างได้นานขึ้น และช่วยลดเวลาในการปฏิบัติงาน (hand-on time)
สำหรับทุกคนที่อายุมากกว่า 2 ปี
T-SPOT®.TB เป็น IGRA เดียวที่ได้รับการรับรองให้ใช้กับเด็กที่มีอายุมากกว่า 2 ปี1
สำหรับการตรวจวินิจฉัยในเด็กนั้น เป็นที่ทราบกันดีว่า ชุดตรวจที่ใช้ทั่วไปกับผู้ใหญ่นั้นอาจจะไม่สามารถใช้ในเด็กได้เหมือนกันกับที่ใช้กับผู้ใหญ่ แต่สำหรับ T-SPOT.TB นั้นไม่เพียงแต่สามารถใช้ได้กับทุกคนที่อายุมากกว่า 2 ปี แต่ยังสามารถใช้กับเด็กที่มีปัญหาสุขภาพอื่นๆ เช่น เบาหวาน หรือ ภาวะภูมิคุ้มกันไม่ปกติได้ด้วย
ติดต่อเรา
To find out more about T-SPOT.TB contact us
Thailand
Biomed Diagnostics (Thailand) Co., Ltd.
1518/4 Kengrungruengchai Bldg.,
7th Fl., Pracharaj Sai 1 Rd.,
Wongsawang, Bangsue, Bangkok 10800
Email: sales-diag@biomedthai.com
Phone: +66 02 5870256 58
Singapore
Oxford Immunotec Limited (Singapore Branch)
160 Robinson Road #23-03
SBF Center, Singapore 068914
Email: enquiry-RoA@oxfordimmunotec.com
Phone: +65 6246 6861
References
- Oxford Immunotec. T-SPOT.TB Package Insert PI-TB-IVD-UK-V3. Abingdon, UK. September 2020.
- Oxford Immunotec. T-SPOT.TB Package Insert TB-PI-US-0001 V9. Abingdon, UK. February 2021.
- Oxford Immunotec. T-SPOT.TB Package Insert PI-TB-IVD-UK-v3. Abingdon, UK. 2016.
- Mazurek GH, Jereb J, Vernon A, LoBue P, Goldberg S, Castro K, IGRA Expert Committee, Centers for Disease Control and Prevention (CDC). Updated guidelines for using Interferon Gamma Release Assays to detect Mycobacterium tuberculosis infection – United States, 2010. MMWR Recomm Rep. 2010; 59(RR-5:1-25.
- Lewinsohn DM, Leonard MK, LoBue PA, et al. Official American ThoracicSociety/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children. Clin Infect Dis. Published online December 8, 2016:ciw694. doi:10.1093/cid/ciw694